


Tools for talking about the hard things
Caring for aging parents in the polycrisis, and how to have conversations that matter

If you like what you read here, please “like” this post using the heart below and restack it on Notes if you get something out of it. It’s a great way to help others find our work.
The best way is to support us is with a paid subscription, starting at just $5 a month!

These are tough times.
The last couple weeks the assaults feel almost innumerable: from the millions of children who will lose school lunch and access to food bank programs, to the attacks on free speech that threaten us all.
The national grief is weighing heavy on many of us right now. And at the same time, the hard stuff in our personal lives and families continue too, especially for those of us in the “sandwich generation” caring for kids as well as aging parents (or spouses, or other loved ones). It can be a lot!
So today I’m offering a conversation I had a few years ago around the anniversary of my father’s death, about how to have better conversations about the end of life. I first published a version of this conversation here.
This conversation left me with this great reminder: The way we live our days is the way we live our lives. And it’s never too soon to talk about how we want to live.
In the months leading up to my father’s death, I had a handful of frustrating calls with the social worker at the hospital where he was being treated. One afternoon, I was standing in a stairwell at my office, asking, “When do we start talking about hospice?” and their answer was confusing and vague, and maybe it wasn’t the right question to ask.
But what do you ask when your dad is facing down death?
Turns out, there are many ways to prepare.
There are death doulas, and podcasts about death, and resources like Re-Imagine, which highlights workshops and end-of-life trainings.
Alongside “death positivity,” there are very practical considerations at hand.
As Dr. Eleanor Feldman Barbera, a psychologist who specializes in elder-care, told me, “People procrastinate…and then there's a crisis. Somebody has a fall, or some sort of health crisis, and then a lot of decisions need to be made in a hurry.”
One way of thinking about it: “Conversations clarify.”
That’s what Kate DeBartolo, the Senior Director of The Conversation Project, told me when we spoke about her work. It’s a program that helps people have conversations about how they want to live through the end of their life.
“We need to normalize these conversations earlier,” DeBartolo told me.
“It's almost easier to talk about it at the end of life if you've been talking about it for the last few decades.”
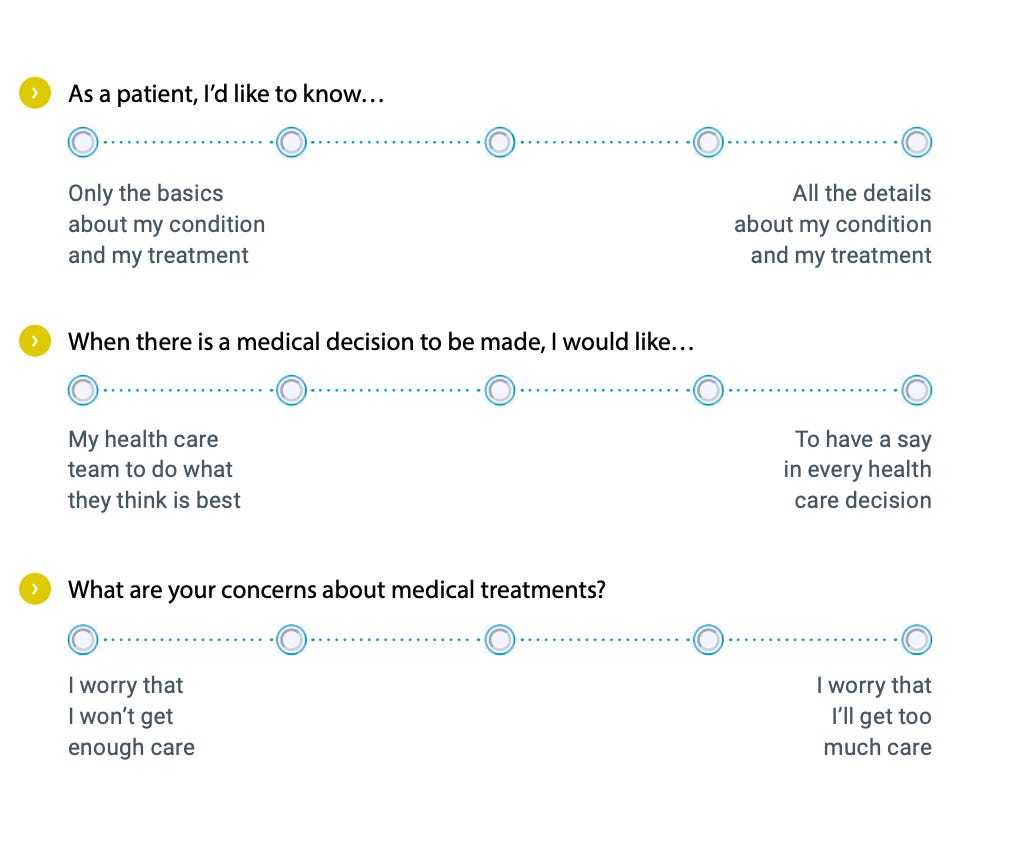
Their “starter” kit offers an 11-page guide to having conversations about what matters to you about your health care.
“What does a good day look like for you?”
“What or who supports you during difficult times?”
“Try finishing this sentence: What matters to me through the end of my life is…”
It also offers guides to choosing a health care proxy, how to talk to a healthcare team, and a guide for caregivers of children with serious illnesses.
DeBartolo and I spoke about the best ways to use their guides. Our conversation has been edited for length and clarity.
One of the questions folks answer in the Starter Guide is: “What matters to me through the end of my life is…”
Why do you start there and what are the kinds of answers you get to that prompt?
We try to start with an open-ended question. It’s not medical; it’s not legal. Just thinking about what matters most to you, and that that can change. You can talk about this again, later, and your wishes can change.
There’s part of a shift in medical care, moving away from “What's the matter with you?” and towards “What matters to you?”
So that might be, “I've got to make it to this wedding in two months,” or “I really need to be able to walk my dog,” or “I can't wait to meet a great-grandchild who's going to be born in three weeks.”
It's so much more about how you want to live your life through the end, and not how you want to die.
We also offer scales when it comes to your medical care: Are you concerned about receiving too much care or too little care? By providing some options – “Where do you fall along this scale?,” it allows people to say, “Oh, I do have an opinion on that.”
Why is it important for to be able to say that to a healthcare provider?
Some people may feel like they want as little pain as possible, or they want to be able to communicate as much as possible, so they’re willing to say, “More pain, but I can make medical decisions.”
Atul Gawande, who wrote Being Mortal, talked to us about how so many patients or family members would come to him and say, “I don't know, Doc, what would you do if this was your mom?”
“[He would say] I don't know your mom. What does she like to do? How important is getting back to ballroom dancing? How comfortable would she be if she's homebound? We need to understand who the person is, rather than what I would want.”
It's maybe a more heartfelt connection to talk about what matters to you, as opposed to, like, “Hey mom, how do you want to die?” There, the answer is, like, “I don't want to die! Conversation over!”
We can't control everything, and we want to be careful about over-promising that if you state these wishes, that they will be perfectly honored exactly as you want.
It's a little bit like birth plans: you can come up with a plan for what you hope will happen. That medically may not be what plays out, but the care team is generally operating under an understanding of what matters to you and and what you want.
And that’s another example of another medicalized process, and people were the ones saying, this is not just a medical experience. This is a life experience, and I've got opinions and thoughts.
So when we have so little control over some things, we can have some conditional control here.
I feel like one reason these conversations are so important now is because science and technology and medicine have gotten so advanced in the last few decades. We didn't used to have as much of a say. If you had a heart attack, or a stroke, or cancer, there wasn't that much that could be done. Now we have a lot of options.
We don't need everybody to be a medical expert. They need to be an expert in themselves and what matters to them.
Sometimes what matters is not having to decide. We know people who are like, “I don't care, I want my kids to make the decision that the time comes.” That is a conversation in and of itself.
To support interviews like this one, become a paid subscriber starting at $5 a month, or gift a subscription to someone else, using the links below.
Thank you so much for supporting our work!
I imagine that there are times when people find certain points to be particularly hard to talk about. How can people get unstuck, if they do get stalled out in this process?
I would start by saying it doesn't all have to happen at once. Especially if you're the one trying to bring it up with someone, rather than forcing it – and especially if somebody is older or frail or sick – really being respectful of what they can handle at the moment.
It doesn't have to be one mega-conversation that you can never revisit.
The pandemic was a great example of that. I remember a gentleman who had told his family and his doctors that he wanted no extreme measures. He was 90-something years old. He lived a good life.
And then he was there in the ICU, with full care, and extreme measures being taken.
And his doctor said, “What's going on, I thought we had a plan?”
And the patient was like, “My first great-grandchild is due in two weeks, and I will do anything to meet that person. Then we can go back to the original plan.”
That, to me, is a perfect example of health systems where people have to be able to be flexible, and that folks' wishes can change.
You talked about birth plans. I'll just say for myself, before I got pregnant, I really didn't know much about childbirth. And I knew almost nothing about death and serious illness until my father got sick. So this work that you're doing is not just about individual conversations, but seems like it’s changing the culture.
We want to normalize having these conversations. We want people to think about their sphere of influence. When you have a friend who might end up in a similar situation [with a sick parent], to be able to share resources with them.
This is one of those things that’s always on the to-do list, that never feels quite as pressing as the thing that really has to get done that weekend.
The age of visitors to our website has gone down a lot over the last few years. I think right now more than half of our visitors are under 45. People who are bringing it up with grandparents, so more intergenerational or skip-generational.
And I find myself drawn to this work, not only for the person at the center, whose wishes we are trying to honor, but even more so lately for the survivors.
If people can grieve the loss of the person, and not all of this extra grief around the uncertainty that went along with the loss, that is what I'm particularly driven by.
If you’re loving MR, give us a like and leave a comment so new readers can find us. Thank you for being here.
MR book club announcement: Do you love reading and talking about books for women, by women? Same. By popular demand we are ramping up book club again, and our next gathering will be in April to discuss Hood Feminism by Mikki Kendall. Come discuss with us and fellow MR readers by becoming a paid subscriber. Bonus: We will be joining the fabulous
for this discussion for twice the feminism :)Past MR book discussions have been delightfully fun and nerdy—see posts here and here to get a taste. Honestly my favorite book club ever! Dates and more details coming soon.
I keep thinking about how we are living under this national crisis, and our personal crisis continue on, too, and it kind of compounds. It feels like a lot! Thanks for this :)
Thanks Allison. It's so good to know about where to turn. I will share this with people in my area who are doing death doula work.